Gonzalo Serrano-Belmar.
@GSERRANOB_MSK • 9,418 subscribers
MSK radiologist at CLINICA ALEMANA SANTIAGO, Chile. Sharing knowledge in a didactic way. Amateur medical illustrator 🇨🇱+🇵🇹 #MSKRad
Shorts

Videos

The Medial Collateral Ligament has a deep component made up of two ligaments—the meniscofemoral ligament (MFL) and the meniscotibial ligament (MTL). The MFL is the most frequently injured, with its most likely site to rupture at the femoral insertion (+/- 80%). The MFL primarily provides stabilization against external rotation. But!!, it also plays an essential role in anchoring the meniscus peripherally, so its rupture may impair the function of the meniscus. Next!! Dynamic Ultrasound!! #mskrad
Gonzalo Serrano-Belmar.72,255 次观看 • 2 年前

Common extensor tendon tear of the elbow. Maximum elbow flexion is extremely useful in better identifying tendon tears. The tears usually have a longitudinal orientation; elbow flexion compresses the tendon like an accordion, opening these longitudinal tears. "BUT," if you see that it opens up a lot with anechogenic fluid, you must have a high suspicion of joint communication. So try to find it! This limits its healing potential. It is a cavern that permanently fills with fluid, preventing its healing. #mskrad
Gonzalo Serrano-Belmar.52,339 次观看 • 2 年前

The soft tissue components of the biceps pulley system include: •Subscapularis •Supraspinatus •The coracohumeral ligament (CHL) •The superior glenohumeral ligament (SGHL) The subscapularis has superficial and deep fibers that envelope the groove, creating the “roof” and “floor”. They also coalesce with those from the supraspinatus and SGHL/CHL complex. They attach at the lesser tuberosity to create the proximal and medial aspects of the pulley system, with soft tissue extensions serving to further envelope the LHBT in the bicipital groove. #mskrad
Gonzalo Serrano-Belmar.52,076 次观看 • 2 年前

Complete rupture of the flexor digitorum superficialis (FDS) tendon 📍 Distal insertion at the middle phalanx, with retraction to the base of the proximal phalanx. 🧗♂️ 20-year-old climber with sudden, sharp pain during climbing. 🔍 Key point of this case: dynamic clinical–ultrasound correlation ▶️ First part of the video (most important): The distal phalanx is actively flexed while blocking the DIP joint. This maneuver isolates the flexor digitorum profundus (FDP), so on ultrasound we should see only FDP excursion — which is exactly what happens. The distal phalanx is flexed without blocking the DIP joint, allowing flexion of the PIP joint. In this situation, both FDP and FDS should normally show excursion. ❌ However, the FDS remains completely still, confirming complete tendon–bone dissociation. ▶️ Second part of the video: 🩻 Final confirmation: • Empty tendon sheath at the expected distal insertion • Retracted FDS tendon stump proximally 🎯 Take-home message: Dynamic ultrasound, combined with proper clinical maneuvers, is crucial to demonstrate functional dissociation and accurately diagnose complete FDS rupture, especially in climbers. #mskrad
Gonzalo Serrano-Belmar.12,452 次观看 • 5 个月前

Continuation of previous MRI case. A 14-year-old boy with persistent discomfort and occasional joint effusion 3 months after a medial knee sprain of the deep component (same injury 3 years ago). We have already seen the MRI. Ultrasound confirms a residual proximal tear of the deep MFL LCM with an insufficient ligament. Dynamic maneuvers with knee valgus in slight flexion demonstrated an insufficient ligament with meniscal hypermobility with the meniscus penetrating the joint with the knee valgus. The deep MCL component STABILIZES THE MENISCUS!! We can provide essential information for decision-making with dynamic US. #mskrad
Gonzalo Serrano-Belmar.40,599 次观看 • 2 年前

Las infiltraciones ecoguiadas pueden realizarse mediante dos técnicas principales: en plano (in-plane) y fuera de plano (out-of-plane). En la técnica en plano, la aguja avanza paralela al transductor, permitiendo visualizar todo su trayecto en tiempo real, lo que ofrece mayor precisión y control. En cambio, en la técnica fuera de plano, la aguja cruza perpendicularmente al haz del ultrasonido y solo se observa como un punto ecogénico, lo que requiere mayor experiencia para ubicar la punta con seguridad. La elección entre ambas depende de la estructura a tratar, el acceso anatómico y la preferencia del operador. Pero también ambas son complementarias al momento de infiltrar bajo guía ecográfica. #mskrad
Gonzalo Serrano-Belmar.20,184 次观看 • 1 年前

Cyclops injury. Also known as localized anterior arthrofibrosis, it is almost exclusively a complication of ACL reconstruction, with the appearance of an ovoid nodule most commonly located on the anterior aspect of the ACL graft near the tibial insertion. Risk factors female gender, greater graft volume, bone avulsion lesions, excessive anterior tibial tunnel, and double-bundle ACLR. This case is a 23-year-old man, a high-level athlete, with limited and painful terminal knee extension post-ACLR. The relationship of the cyclops lesion with the limitation of the knee extension during flexion-extension maneuvers can be observed. Undoubtedly, magnetic resonance imaging of the knee is the imaging study of choice. Still, dynamic ultrasound can be an excellent complement to demonstrate to the patient and treating physician its causality. #mskrad
Gonzalo Serrano-Belmar.36,889 次观看 • 3 年前

FOR THOSE INTERESTED IN THE SUPRASCAPULAR NERVE CASE AND HOW TO LOCATE IT. Normal Anatomy: To TRACK the SUPRASCAPULAR NERVE with ultrasound, start at the supraclavicular fossa. A high-frequency linear probe is used to identify the SUPERIOR TRUNK of the brachial plexus, which is seen as a “honeycomb” structure BETWEEN THE ANTERIOR AND MIDDLE SCALENE MUSCLES. Locate the suprascapular nerve as a small branch from the superior trunk, then follow it laterally and posteriorly beneath the OMOHYOID MUSCLE. Continue tracing it toward the suprascapular notch, which passes under the superior transverse scapular ligament. KEY LANDMARKS include the scapular spine and coracoid process. Look for signs of hourglass constriction, such as nerve flattening, hypoechoic areas, or fascicular swelling. Proper alignment and dynamic scanning are essential for clear visualization. #mskrad
Gonzalo Serrano-Belmar.22,521 次观看 • 1 年前

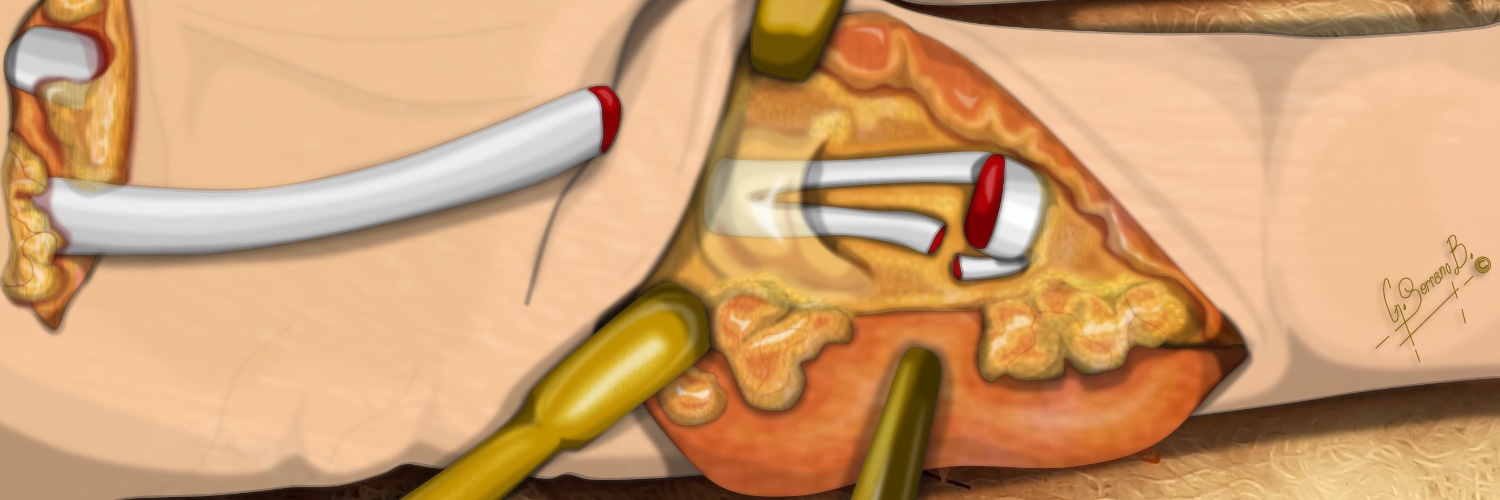
Morton's neuroma occurs at the terminal bifurcation of the common plantar digital nerve. The deep transverse metatarsal ligament connects the metatarsals. Below the ligament, we find the nerve, and above the ligament, the bursa. And distal to the anterior free edge of the ligament, the neuroma. It is at this level that the nerve makes a pronounced dorsal turn at the distal free edge of the ligament. We can see this demonstrated in the video/illustration. This explains one of the theories; entrapment between the plantar soft tissues and the ligament. The dorsal approach for me is the best 👍 . We avoid the thick plantar skin. Compressing with the finger on the plantar side and sliding it also lets us differentiate the distinct components, where the ligament remains immobile. We can also mobilize the nerve and see how it imprints against the anterior free edge of the ligament, understanding the pathomechanism. Finally, the Mulder maneuver always helps. #mskrad
Gonzalo Serrano-Belmar.36,698 次观看 • 3 年前

Instability of the long head of the biceps tendon (LHBT) is almost always associated with other shoulder pathologies, mainly pathology of the rotator cuff (supraspinatus and subscapularis tear). Therefore, every time we find RC tears, we must explore the stability of the LHBT. The most critical stabilizers are the SGHL, CHL, and the intertwining fibers of the supraspinatus and subscapularis. Here is a case with a high-grade subscapularis tear with continuity of the most superficial fibers/transverse humeral ligament that limits retraction,associated with medial dislocation of the LHBT. With an extension, abduction, and internal rotation maneuvers of the shoulder, we reposition the tendon in the bicipital groove, with subsequent re-dislocation due to external rotation, showing a marked exit snapping, very painful. We can add important dynamic information. #mskrad #MedTwitter
Gonzalo Serrano-Belmar.31,636 次观看 • 2 年前

MRI guide to locate the inferior calcaneal nerve, first branch of the lateral plantar nerve (Baxter’s nerve). There are three possible entrapment sites: 1. Deep or adjacent to the fascial border of a hypertrophied abductor hallucis muscle. 2. Along the medial border of the quadratus plantae muscle. 3. Adjacent to the medial calcaneal tuberosity. Next, US. #mskrad
Gonzalo Serrano-Belmar.30,492 次观看 • 2 年前

Degloving injury Separation between the inner and outer components of the RF muscle is demonstrated by the mobilization of the minimal amount of fluid at the interface by muscle hand-squeezing Substantial difference in prognosis between a partial and a degloving injury #mskrad
Gonzalo Serrano-Belmar.27,308 次观看 • 3 年前

Intrasubstance medial delamination extension of the supraspinatus tendon can be difficult to assess on US, MRI, and arthroscopy. “Water” (bursal or articular) is always an ally for exploration. We force the entry of bursal fluid towards the laminar delamination of the tendon, distending it slightly but enough to identify it. #mskad
Gonzalo Serrano-Belmar.21,111 次观看 • 2 年前


Persistent/ Recurrent trigger finger after a release of the A1 pulley. Triggering occur between the noose formed by the two slips of the FDS and the FDP at the Camper’s chiasm at the distal edge of the A2 pulley. Always check for other possible points of conflict. #mskrad
Gonzalo Serrano-Belmar.22,983 次观看 • 3 年前


Quick case. Coronal view. Signs of disruption of the fibrous septa and subluxation of the plantar calcaneal fat pad with compression of the ultrasound transducer, reproducing a snapping of the fat pad. Bibliography reference. Skeletal Radiology Skeletal Radiology #mskrad
Gonzalo Serrano-Belmar.15,515 次观看 • 2 年前

没有更多内容可加载