Video yükleniyor...
Video Yüklenemedi
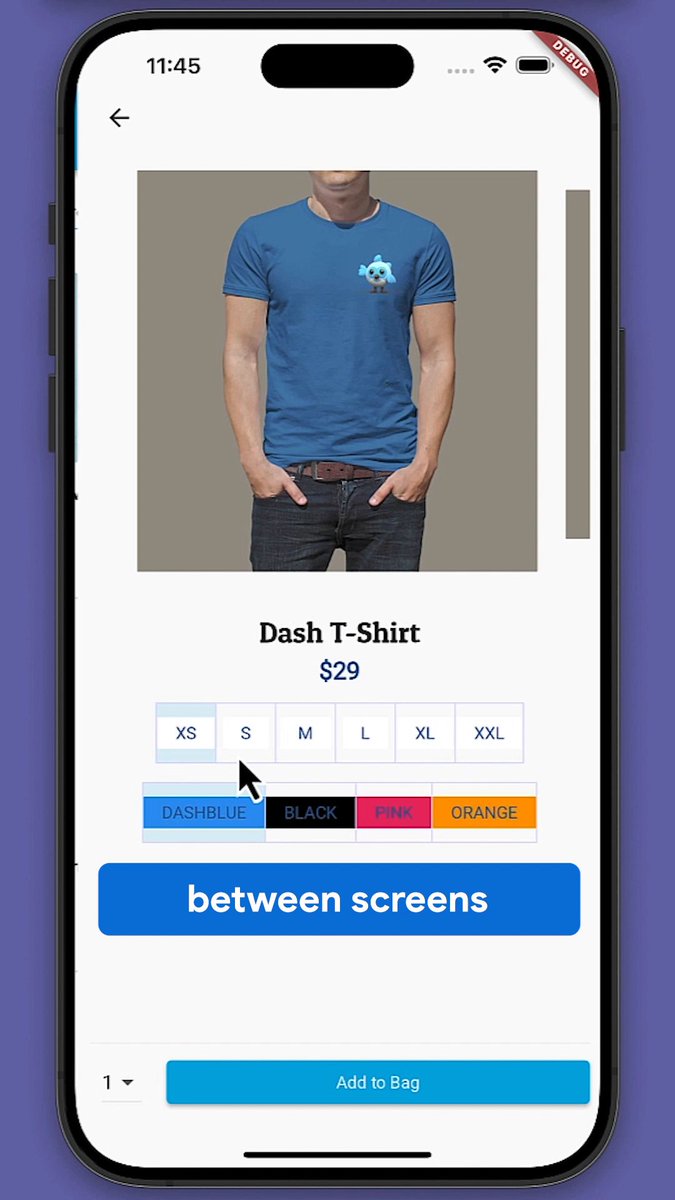
Snaring an adherent clot should use the same strategy as snaring a polyp. Make sure you get max capture on the first grab. #GITwitter

35,371 görüntüleme • 2 yıl önce •via X (Twitter)
11 Yorum

I always worry about what is underneath!

Why would you remove an adherent clot that’s doing its job??? All I hear in my head is the song “danger zone“

In order to treat it more durably endoscopically. The rebleeding rate is fairly high 25-30% if left alone. Guidelines leave it ambivalent whether to do this or not.

That’s a stress test for the endoscopist right there 😳

Beautiful demonstration of this technique!

You go with a cap right from the start for every bleeder?
Not always, only if I am suspecting DU. No hematemesis Melena , high BuN /Cr +NSAIDS

@EndoCollabcom 😳😳 Given how the guidelines are vague, is it your practice to always remove an adherent clot and be prepared to treat what is underneath or does it really situational?
@EndoCollabcom I almost always remove the clot and treat as I am prepared if I upgrade it to active GIB and have back up (Hemospray/IR)

.@DrBloodandGuts what cap are you using in this video?
Olympus
Benzer Videolar

Sensitive content
As a guy, always make sure you smasħ on the first date so you don’t lose both your money and the meať pie
fimlex
724,388 görüntüleme • 9 ay önce




Sensitive content
Do what works for you, but make sure you're on the same page. Take the time to really get to know the person and put in the effort to make it work.
Larkin Love
23,165 görüntüleme • 1 yıl önce