

Evandro Martins F. MD
@evandrofilhobr • 20,642 subscribers
🇧🇷 Interventional Cardiologist | #RadialFirst #CTO #ImageFirst | Complex PCI & Structural Heart | Sharing cases, science & passion
Shorts



Videos

Protruding aorto-ostial stents can preclude safe TAVR. The RASE technique, integrating reverse hairpin re-entry, intentional fracture & snare extraction, offers a out-of-the-box controlled solution. Honored to contribute to this work in JACC Journals Case Reports with Raghav Gattani et al.
Evandro Martins F. MD21,286 просмотров • 12 дней назад
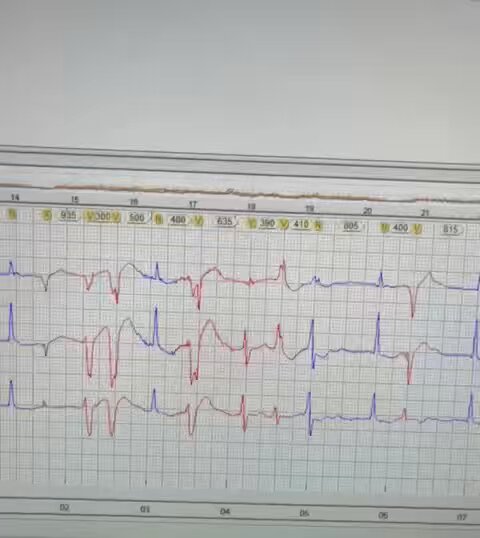
Patient at home using a 24h Holter monitor. Trace reading after his death.
Evandro Martins F. MD67,427 просмотров • 1 год назад

RCA CTO w/ ambiguous proximal cap. Knuckle wire advanced subintimally and probably inadvertently tracked an RV marginal branch, exploding... Luckily, perforation was into the RV cavity. No pericardial effusion, no tamponade. No need this time but always have echo + pericardiocentesis kit ready.
Evandro Martins F. MD14,580 просмотров • 3 месяцев назад

Shocking news. Looks like Damar Hamlin suffered a commotio cordis. Hope he recovers asap.
Evandro Martins F. MD89,541 просмотров • 3 лет назад


85F. Double occlusions RCA & LAD. CMR with heavy burden ischemia. Target was RCA, 1ry retro due px cap ambiguity using AV epicardial channel. Device uncrossable lesion after wire IP crossing. Grenadoplasty. IVUS & CB for plaque modification.
Evandro Martins F. MD15,697 просмотров • 8 месяцев назад

Tip for the #calciumcrackers using Shockwave Medical I’ve been prepping the SW balloon the same way I do w/ Stingray balloon. Very fast and effective. - 20cc empty luer lock syringe for vaccuum generation - 3cc luer lock syringe with pure dye - simple stopcock (blue one is my favorite) Don’t do negative pressure with indeflator before the first insuflation.
Evandro Martins F. MD40,658 просмотров • 2 лет назад



16👨🦰, complex ASD anatomy (very floppy rims, aneurismatic septum >10mm, absence of aortic rim). Failed attempt of percutaneous closure. ASD18 embolization (33/29 LA/RA discs) to the aortic arch. Successful snaring from the pin-hub after 2h trial. Upsized to 16F arterial sheath.
Evandro Martins F. MD35,171 просмотров • 3 лет назад

One of the great cases we’ve done in our 2 days CTO Club 2025 meeting. Crazy ostial LAD CTO w/ severe parietal calcium and aneurysmal morphology. Antegrade approach using Power Puncture of px cap w/ H14 followed by AW w/ H14 after failing AW Gladius > GN3. Also tried HDR. 4.0 IVL & 2 Megatrons 4.5 & 5.0.
Evandro Martins F. MD15,797 просмотров • 1 год назад

Sometimes we must take calculated risks to achieve good outcome — as long as every step is carefully planned. 🔹 Proximal LAD CTO opened retrogradely through patent LIMA. 🔹 Distal LAD collaterals used for RCA CTO retrograde recanalization. When there’s no easy way, build one!
Evandro Martins F. MD10,938 просмотров • 11 месяцев назад


Have you ever had? How to solve it? How to prevent it? This is a case of stuck “jailed” guide-wire due to the formation of knot on itself during attempt of wire removal in a provisional bifurcation PCI. During trials of wire removal the wire coil unraveled and detached followed by fracture of the core in a more proximal segment. PS: Wire fragment was left alone due advanced patient age and risk of stent deformation during attempt to snare it.
Evandro Martins F. MD15,160 просмотров • 1 год назад


RCA aorto-ostial - ISR CTO with older overhanging under-expanded stent. Impossible to engage with any guide. Retro through septals w/ Mamba Flex 150. Samurai RC. Retro crossing with Hornet 14 (2x). MC uncrossable. Tip in H14 into JR in aortic arch. Trapping. Externalization. Undilatable ostial lesion. 3.5 & 4.0 balloon rupture 30 ATM. Wolverine 4.0 - 22 ATM. 4.5 balloon 32 ATM. MLA from 2.2 -> 6.1 mm2. No SW available, unfortunately.
Evandro Martins F. MD21,993 просмотров • 3 лет назад

Probably my most challenging case this year… RCA ISR CTO - AW Corsair Pro 135 w/ Gladius / GN 3 / CP12 / Astato 20. Poor progression (15mm progression in 1 hour attempt). Very very fibrotic. GZ 7F. 1.25 / 2.0 balloons (rupture). Retro through S1. Mamba Flex & Sion Black to PL. Puncture to stent with GN3. No progression. Abandoned S1. Apical epicardial channel. Mamba Flex & Sion Black. Changed to Finecross. J wire technique to for channel crossing. Gladius & Pilot 200 & GN3 & CP12 & Aststo 20 for RWE couldn’t go inside stent. Knuckled gladius outside stents. CP12/Astato for RW. GZ assisted RCART and failed. Fresh H14 crossed to aorta. Snared H14 but locked inside the guide catheter, hard time to free the wire locked onto snare. H14 unlocked. Finecross stucked but finally after new attempt could traverse to aorta. R350 snared in brachiocephalic trunk. 4 DES. 1 DES stripped. 3.5 & 4.0 NCs. IVUS
Evandro Martins F. MD18,702 просмотров • 2 лет назад



84🧑🌾, CCS IV angina despite all the OMT you can imagine. CABG turndown. 3VD (2 CTOs RCA-LCx & calcified LAD). MRI all viable territories, EF 40s. High-Risk PCI to the left system w/ IABP support. Giving some hope to the ones most in need. Superseletive OM injection, ping-pong guides & #IVUSguidedADR
Evandro Martins F. MD19,455 просмотров • 3 лет назад