James Noake
@DrJN_SportsMed • 34,200 subscribers
Difficult stuff. Consultant in Sport, Exercise & Musculoskeletal Medicine
Shorts




















Videos

Consent ✅ Retired nurse, 60s Decade of flank / loin pain - perceived around thoracolumbar junction (blue cross) Extensive MSK, renal and GI investigations - no diagnosis forthcoming CT and MRI of spine reported normal On systematic palpation / PA glide in prone, her pain is actually provoked more inferiorly (green cross) POCUS video - calcific changes at 12 rib interface with spine, correlating with her pain - there is no true costotransverse joint at this level, rather ligamentous attachments- so this represents an enthesopathy / 'ligamentopathy' US guided LA & CSI - complete abolition of pain after 10 years! (see enthusiastic gyrating - sound on)
James Noake50,255 views • 3 months ago

updated imaging 🤔🤦😆 MRI sagittal then axial CT sagittal then coronal
James Noake20,633 views • 1 month ago

Consent✅ So - how many times do I have to say this? This is close to my 200th case - medial neck of femur stress injury, in a runner who is over-training, misdiagnosed as a 'hip flexor' problem 🤮🤢 Look at the video & appreciate why the 'hip flexor' might be implicated
James Noake66,280 views • 7 months ago

Consent✅ "I’m at the Point of Breaking – Hang 10, take it thighs-an easy, I’m Hunting for a solution" Runner, surfer Massive ramp up in marathon training – rapid onset medial mid to lateral burning thigh pain (see pain map below) with low grade parasthesiae Exacerbated by deep knee flexion and running beyond 20 mins and a faster pace Struggled further on surfing holiday in prone on board and kneeling MRI excluded femoral bone stress injury and no adductor injury or knee intra-articular / ligamentous injury OE – Meniscal and ligamentous testing normal Lumbar spine and hip joint cleared POCUS video reel – Adductor magnus tendon & wider musculature normal Saphenous nerve swollen at mid Hunter’s canal point – almost same calibre as the adjacent femoral artery! (point of maximal tenderness with probe pressure - Tinel's positive) US guided hydrodissection (LS) – soft tissue planes around SN seen to open up effectively Post procedure – complete abolition of pain on treadmill running and deep squats for the first time in 8 months (excuse the language) Pearls - This area is diagnostic ‘No Man’s Land’ – ie, if there is no femur bony pathology, and in the absence of trauma, it can only really be neural ‘Adductor splint syndrome’ – a form of bone stress injury – is one of the key medial thigh pain differentials in runners Research links – ‘Surfer's neurapraxia - an uncommon surfing injury of the saphenous nerve’ ‘Adductor insertion avulsion syndrome (thigh splints): spectrum of MR imaging features’
James Noake16,564 views • 1 month ago

0:30
Sensitive content
This media may contain sensitive content.

Consent ✅ Professional race driver - FIA endurance / LeMans R upper limb heaviness, weakness, headaches and facial pain with very high sustained effort in car over 3-4 hours - specifically repetitive shoulder abduction, forward flexion, rotation Pre-dated by high energy 'whip lash' injury in crash Numerous cervical spine investigations abroad - all normal Most telling exam sign - Roo's test - (see video reel) Forearm and hand cyanosis with vein dilatation Highly suggestive of vascular (venous thoracic outlet syndrome) End of reel - duplex ultrasound shows flow occlusion taking patient into functional driving position (FF, lateral raise 60 deg max) Awaiting MRI TOS protocol with contrast and arms up / down vTOS can be caused by myriad anatomical variants - anomalous muscle slips, ligaments, accessory rib, and also post trauma Pearls - listen to the patient, the story's the pattern, and the sporting MOI
James Noake21,014 views • 2 months ago

Documented consent ✅✅ Super fit male 70s Extreme skiing, climbing Previous lumbar fusion, then discectomy L4/5 Lost sporting confidence, with insidious drop off in functional power & coordination in R > L legs Dragging foot Leg doesn’t “feel like my own & it spasms unpredictably” Can’t heel or tip toe walk - no lower motor neurone signs as one might expect in context of previous surgery… Rather, marked UPPER motor neurone signs (see video - clonus +++ and hypertonicity) Whilst examining lower limbs supine on bed - “What are these abdominal scars?” “I had an appendicectomy” “What about these ones? (port scars - look closer) “Oh yes, i had a radical prostatectomy for cancer several years ago” MCC (cord compression) now top of the differential diagnosis list. Tips: 1. Always expose the patient as fully as is appropriate 2. Don’t automatically assume patients will report all the relevant medical stuff even if you ask “any other medical conditions I need to know about?”
James Noake50,194 views • 1 year ago

Consent✅ Female, 20s L upper abdominal pain since lockdown - on back of increased home work outs including ab & core work Now pain lying supine, prone, trunk rotation, being hugged, deep inspiration.... Hugely impactful on QoL Seen multiple specialists - GI, gynae (!), respiratory - utterly frustrated Referred as possible ACNE syndrome - but not in the right place anatomically (ACNE is peri-umbilical semilunaris border) OE - hypermobile ? EDS Focal pain on gentle palpation into immediate L inferior costal margin EROM thoracic rotation painful, plus trunk flexion / extension POCUS video - L 'floating rib' - possibly 11th - seen subluxed superficially over adjacent rib, vs normal side sat 'flush' On deep inspiration, pain reproduced with probe pressure maintained as irritable over-lying soft tissue 'tents' Diagnosis - 'Floating rib' or 'rib tip' syndrome Outcome - symptoms validated - no more medical 'rabbit holes' - surgical resection
James Noake24,669 views • 7 months ago

Consent✅ Another - possible - genicular nerve case Runner, bilateral lateral knee pain Treated as ITB overload; exhausted all non-surgical options so reasonably proceeded to targeted partial ITB release Unfortunately symptoms persisted but changed in nature - 'burning' now (L more than R), slightly more diffuse & symptoms with sitting, not just on exercise POCUS video - Scarred thickened ITB (typical post-surgical legacy) seen, with superolateral genicular NV bundle sat just deep to it Injection - hydrodissection of scar tissue around the NV bundle, freeing up the fascial plane systematically - hard work because of the density of the tissue Post procedure (volume up) - patient essentially pain free on the treadmill - R side (not injected) still painful
James Noake19,381 views • 7 months ago

Consent✅ Runner, HIIT Deep left buttock pain Occasionally travels down posterior thigh with intermittent parasthesia & numbness lower leg & foot Brought on with pigeon stretching, yoga, as well 4 point kneeling core hip extension / adduction work 🤷♂️ Sitting main aggravating factor - isometric single leg bridging as well Clinical exam difficult to reproduce pain but discomfort on palpation through deep gluteal space MRI: Lumbar spine - normal Pelvis - mildly reduced ischiofemoral interval L side - subtle oedema in quadratus femoris (QF) POCUS video: With passive hip external rotation (closing down the ischiofemoral space) can see bunching of QF and tenting of sciatic nerve (SN) - 'Eruption Sign' - maintaining probe pressure on this soft tissue during the manoeuvre reproduces typical pain US guided injection (lateral to medial to avoid SN) to QF and ischiofemoral space - immediate reduction in sitting pain post procedure
James Noake16,304 views • 6 months ago

Consent ✅ Footballer - ACL recon & MCL tear 12 months ago Uneventful rehab process & RTP ...... but then developed focal pain over medial joint line & restricted flexion Sore on side passing & cutting / change of direction drills OE - Palpation pain at proximal MCL Stiff & painful into EROM flexion MRI - no medial pathology reported - but on closer inspection, subtle medium signal focal change in deep MCL on T1 & T2 (always check the scan yourself) POCUS - obvious large heterotopic calcific deposit in previously injured proximal MCL fibres - Pelligrini-Stieda lesion Video - needle barbotage / fenestration of deposit, finished with a soupçon of CSI 🫰 Post procedure, complete abolition of pain in gym & typical provocative movements ✅ Ultrasound is much better than MRI in identifying calcific pathology (as is plain x-ray)
James Noake20,172 views • 8 months ago

Consent✅ Lots to think about here Male, 40s- super fit - skiing, running, weights Always had stiff hips and tight 'hip flexors' 👀 hmmmm Recalls aggressive breaststroke kick right side (ie minimal trauma) - sudden catching pain right groin Remained intrusive with mechanical symptoms - pain at rest, sitting, rolling over, deep squat Exam - both hips reduced ROM especially into FADDIR -right particularly irritable Video - AP Xray pelvis - bilateral dysplasia R > L, plus cam bumps.... a hip pain 'perfect storm' POCUS - extensive R sided delamination labral tear (use passive hip rotation to manipulate & 'milk' effusion fluid into tear to highlight it) MRI images (surrogate markers of dysplasia) 1. 'Saturn Sign' (I made this up) - anterior to posterior labral tear 2. Cystic change in ligaments teres 3. Hypertrophic cystic labral changes It's not just women that have dysplastic hips This needs experienced surgical input rather than 'kicking the can down the road'
James Noake14,346 views • 6 months ago


14 day post op Maia implant update Basically looks & moves like a normal thumb
James Noake42,544 views • 2 years ago


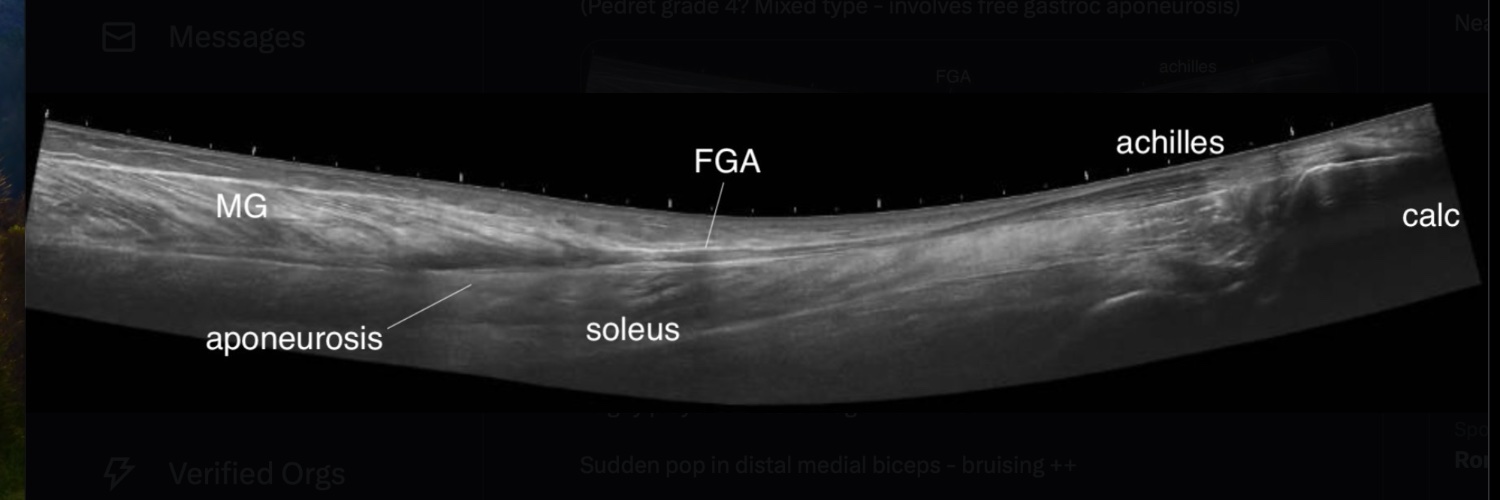
Consent ✅ Teen runner & footballer - mid thigh pain after intense Sport's Day culminating in hard 800m couldn’t recall acute pop / tear then recurrence during 'Duke of Edinburgh' award hiking with back pack Kicking & sprinting provocative ++ POCUS - rectus femoris tear adjacent to posterior aponeurosis (BAMIC 2A?) - small haematoma Central tendon not involved - but given recurrent nature, I'd tend to be conservative with RTP timescales eg 6 weeks plus Interested in others thoughts... carlespedret
James Noake39,730 views • 3 years ago

Consent✅ ACL reconstuction with lateral tenodesis 9 months ago Persistent lateral pain 'sliding / catching' sensation over tenodesis site on predictable knee flexion squat angle Tenodesis screw looks ok on x-ray POCUS - fluid / inflammation seen around graft as passes under LCL (graft = circle.... then narrow slip as US turns longitudinal) @orthotwitter - do you see graft / tenodesis soft tissue irritation - impingement? - in any of your cases?
James Noake25,895 views • 2 years ago

Consent ✅ Middla aged Ironman Months of L inferior gluteal pain that radiates into posterior thigh to knee - burning / throbbing Recent 'pop' in gluteal region with sudden hip & lumbar flexion Worse on - running / fast walking, sitting, cough / sneeze +ive proximal hamstring tendinopathy tests +ive adductor magnus bias tests +ive SLR neural tension Pain LSp flexion, limited POCUS & MRI - interface tear (peel away lesion) of proximal hamstring but remaining tendons intact, so no retraction LSp MRI - L sided disc bulge irritating L S1 nerve root So - concurrent pain drivers? Or one injury mimicking the other? PHT pain can refer pain distally into hamstring. What next after 3 months rehab / load mods & no change? 🧐 Patient will return with symptoms provoked - then US guided LA only injection to proximal hamstring tendon - then re-test - easier & safer to rule out / in tendon driven symptoms first before considering spinal options.
James Noake19,433 views • 1 year ago


Consent ✅ Female early 20s - overweight Started running for weight loss Bilateral cramps medial gaiter area & ankle pain Complains of 'swelling' in the region Pain settles quickly post exercise after 30-60mins More recently P&N spreading into plantar aspect of foot Video slide show - MRI shows hypertrophied FHL muscle belly & very low lying, down to level of sub-talar joint Now causing tarsal tunnel symptoms - tibial nerve (with high signal / mild oedema) immediately adjacent to FHL muscle belly Low lying / accessory soleus can also behave like this Consider gait re-training, optimising triceps surae capacity to 'offset' FHL, botox, US guided targeted tarsal tunnel hydrodissection injection, de-bulking of muscle as last resort if conservative measures fail
James Noake12,853 views • 1 year ago

Consent ✅ Very interesting case!! 🤓🤓🤓 Young teenager - laparoscopic cholecystectomy months ago Persistent debilitating R upper quadrant pain around port scar site Burning, stabbing - provoked by minimal activity eg sitting up, bracing in car turning corners 4 weeks as in-patient in hospital, having further general surgical work up .... MRI, US, CT, bloods normal Off school Examination - +ive Carnett's sign, pain / inhibition on sit up, clearly abdo wall issue POCUS - can appreciate subtle port site hypoechoeic channel through rectus abdominus - this has injured the anterior cutaneous nerve at this level (T9 / T10 - see ACN schematic) Video - US guided nerve block / hydrodissection..... immediate pain relief 🥳 So at least the potential (harmful) hunt for a non MSK / gastroenterological cause can stop now Only one other case report of this in 2022 - but not a typical laparoscopic complication or tick box form. If the block fails to improve pain beyond short term, RF ablation might be helpful - then last resort surgical neurolysis.
James Noake15,558 views • 1 year ago